One of the most common requests in aesthetics is the removal of ‘Brown spots’ and other pigmented lesions. Because all pigmented lesions contain the light absorbing pigment melanin, lasers are often used to selectively target pigment, whilst sparing surrounding normal structures.
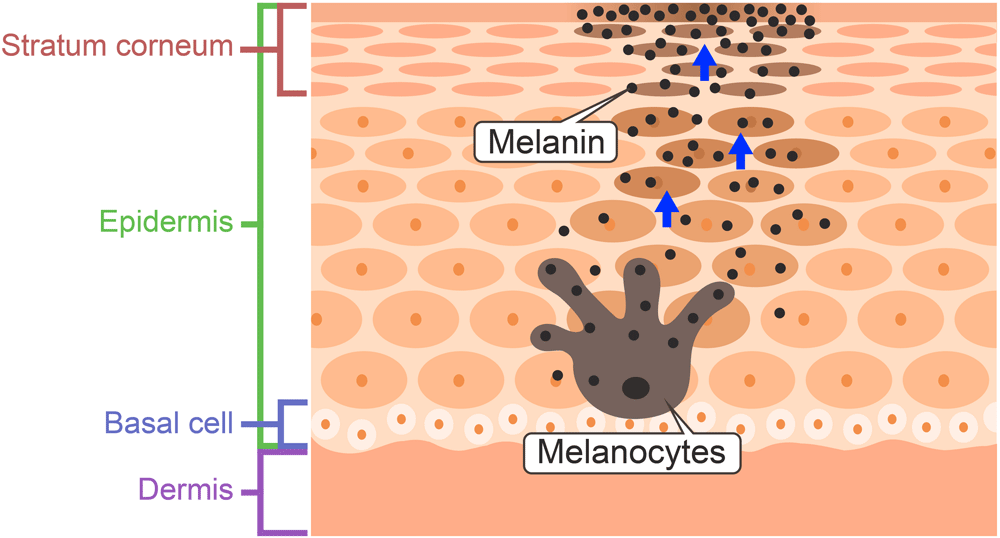
Melanin is produced by specialist skin cells within the epidermis called melanocytes. These cells insert granules of melanin into tiny structures within the cell called melanosomes. Melanocytes are branched cells with finger like projections. As the melanosomes mature, they migrate to the tips of the projections and are transferred into the surrounding skin cells.
The complex choice of which laser to use in the treatment of a pigmented lesion is often taxing for the most experienced laser physician. It depends on numerous factors including the type and depth of lesion, its size and location, the patient’s underlying skin type and other variables.
By selecting the appropriate laser wavelength (colour) and pulse width (dwell time) a pigmented lesion can be destroyed with little or no injury to normal surrounding skin.
Effect of pulse width (dwell time)
The time a laser beam remains or dwells on a particular area is very important. Medical lasers deliver energy in pulses, typically in the picosecond (ps), nanosecond (ns) or millisecond (ms) range. A pulse of light with a wavelength absorbed by the pigmented lesion that dwells on the target just long enough to heat the target, cutting off before any heat is allowed to transfer to normal adjacent tissue, will destroy the target and spare the surrounding structures. The pulse width needs to shorter than the thermal relaxation time (the time required for an object to cool to half the temperature) of the structure. The length of the pulse width is roughly proportional to the size of the target.
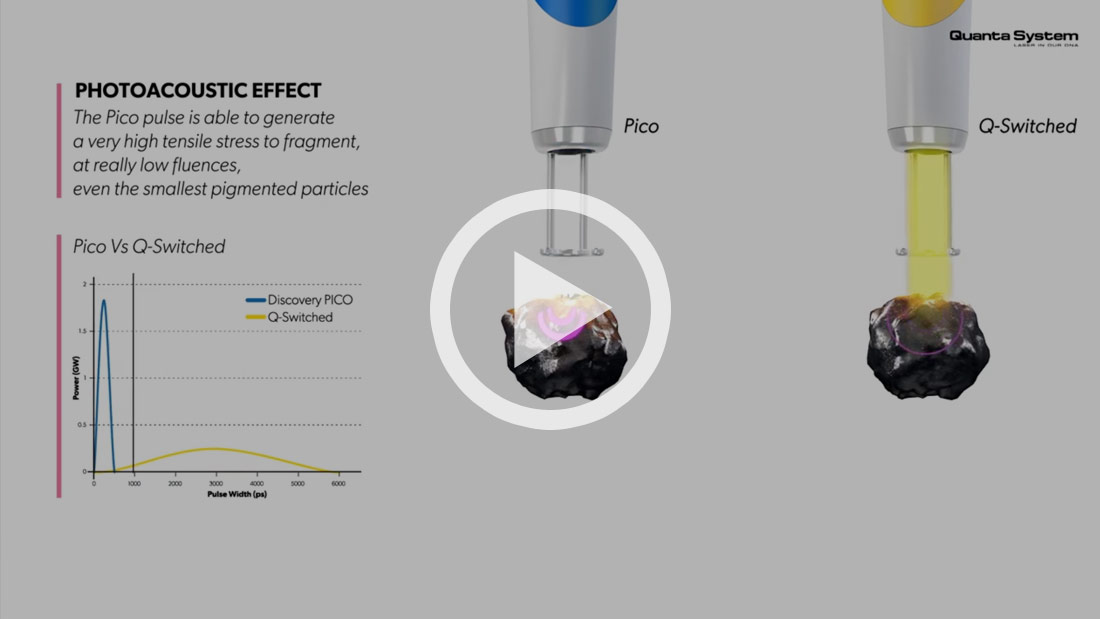
If the target is very small (intracellular melanosomes) a Pico laser with a pulse width of trillionths of a second will best match the thermal relaxation time, destroying the stored pigment, leaving the melanocytes which are producing the melanin relatively undamaged. Slightly larger structures will respond well to photo-thermal Q switched laser with a pulse width of billionths of a second. Pico lasers are more photo-mechanical and produce less collateral heating of surrounding structures. This makes them ideal for the treatment of pigment problems in darker skin types.
When the aim is to destroy larger melanin containing cellular structures a millisecond pulse laser will best match the thermal relaxation time, allowing the heat energy to spill over from the stored pigment into the surrounding melanocytes and keratinocytes causing more extensive thermal damage.
If the pigmented part of the lesion is bulky or above the surface of the adjacent skin, a laser with a non–selective thermal effect such as the Er Yag 2940nm laser or CO2 10,600 nm laser might be the most appropriate choice.
The effect of wavelength (colour)
Several different laser wavelengths can be used to selectively treat pigmented lesions, including green (KTP 532nm laser), yellow (PDL 595nm laser), red (Ruby 694nm laser and Alexandrite 755nm laser) and infrared (Nd Yag 1064nm laser).
Other components of the skin (blood and protein) also compete with melanin to absorb laser light, and as a result, shorter wavelengths (KTP 532nm and PDL 595nm laser) do not penetrate the skin as deeply as longer wavelengths.
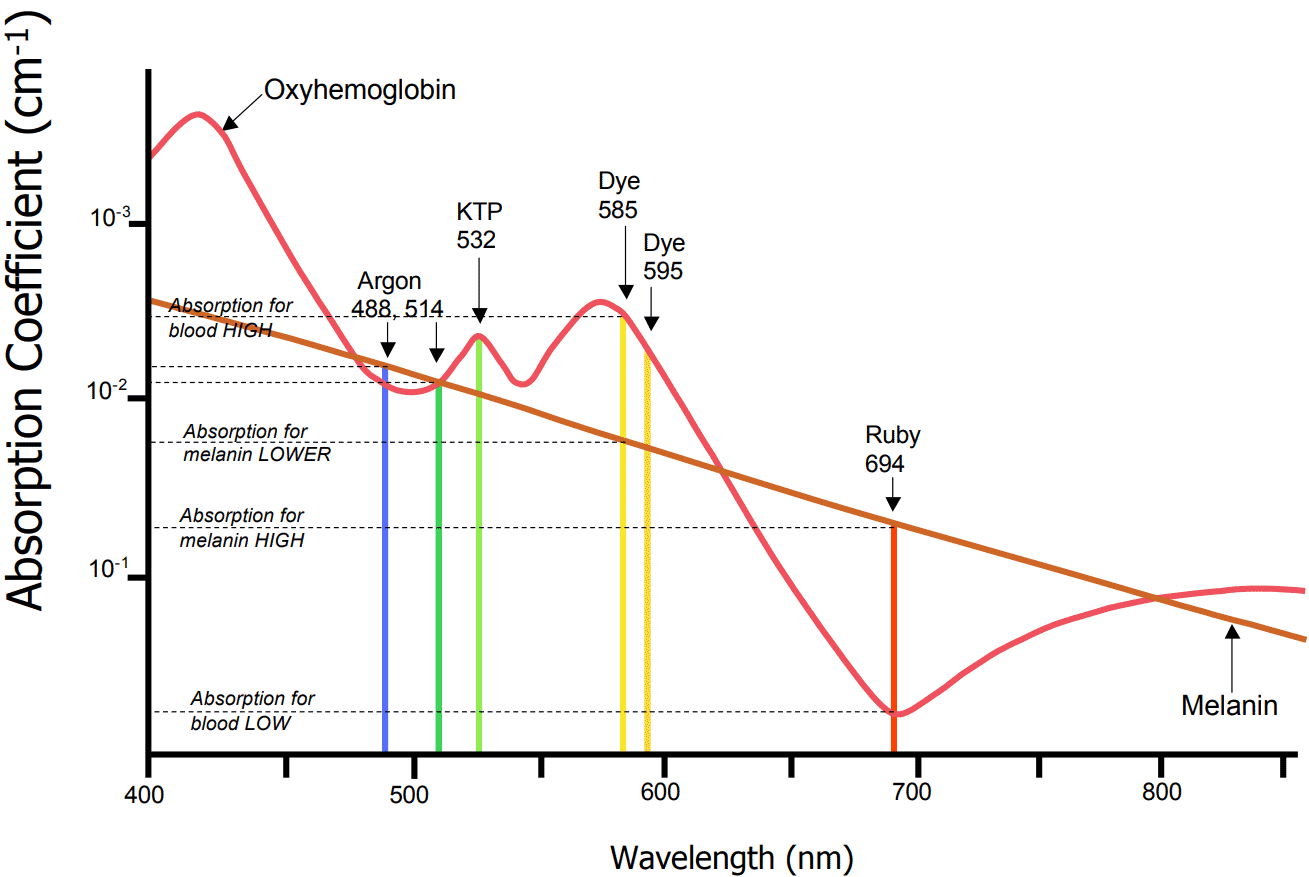
A useful therapeutic window of wavelengths exists between 630nm – 1100nm where melanin absorption exceeds that of haemoglobin and laser light penetrates deeply.
As the absorption of melanin falls as the wavelength increases, higher fluences (power) are required at longer wavelengths to produce the same damage to the melanosomes.
To complicate matters, melanin normally present in the skin may compete with the melanin in a pigmented lesion, which can further limit the choice of wavelength in a given patient. The depth and relative content of melanin in the skin and pigmented lesion determines which laser wavelength is most appropriate for a given patient.
Our Cambridge Laser Clinic offers the complete range of laser and light technologies best suited to treat pigmented lesions, ensuring optimal results.
- Ruby 694 nm Q switched laser
- Alexandrite 755nm LP laser
- KTP 532 nm Pico / Q switched / Opti-Pulse laser
- Nd Yag 1064nm Pico / Q switched laser
- IPL 540 – 950nm light source
- IPL 570 – 950nm light source
- Er Yag 2940nm laser
- C02 10,600nm laser
The two major factors controlling the choice of laser are a) Lesion contrast and b) The underlying skin colour. As a rule, the following choices are made:
| Degree of contrast between lesion & background skin colour | Laser wavelength & Pulse Width recommended |
| High level of contrast (the lesion is very dark and the surrounding skin is much lighter) in lighter skin types (Fitz I-III) | Alex 755nm in long pulsed mode |
| Medium level of contrast (the lesion is dark and surrounding skin lighter) in lighter skin types (Fitz I-III) | Ruby 694nm in Q switched mode KTP 532nm in OP mode (especially if co-presence of vascular markings) |
| Low level of contrast (lesion and skin are close in colour) in lighter skin types (Fitz I-III) | KTP 532nm in Q switched or Pico modes |
| High level of contrast in darker skin types (Fitz IV-VI) | Ruby 694nm in Q switched mode |
| Medium and Low levels of contrast in darker skin types (Fitz IV-VI) | KTP 532nm in Pico mode |
Most clinics have only the choice of IPL or one laser wavelength. Results will be inferior to a clinic that has multiple laser options and an operator who fully understands the strengths and weaknesses of each technology.
To complicate matters further, Pico lasers can be High or Low quality and Q switched lasers can be Active or Passive. The differences are explained below:
Pico Lasers
These lasers can be split into 2 camps – High-Quality Pico & Low-Quality Pico
A High-Quality Pico utilises a seed laser to interfere with an actively Q Switched treatment beam. Light is used to control light delivering a fixed pulse width or shutter speed (in our laser 350ps KTP or 450ps Nd Yag) at a high energy of 800mj.
A Low-Quality Pico utilises older repackaged Q switched technology and runs the Q switch faster – electronics controls light producing an unstable fluctuating pulse width or shutter speed that cannot be faster than 500ps and becomes longer as the fluence increases. The max power output is only 400mj.
Half the power at a wider pulse width equals low power, slow results and disappointing clinical outcomes.
Active Q Switching
Our active Q switched lasers have the ability to deliver a single high-energy pulse. This is important because only the 1st pulse is able to shatter the pigmented lesion, leaving water vapour behind forming a frosted white appearance.
This frosted white reaction forms an impenetrable optical shield. If additional pulses are stacked in the same area they will only have the unwanted effect of over heating the skin resulting in thermal damage.
Passive Q Switching
Most of the laser technologies advertised for pigment removal are cheaper lasers that produce a train of smaller pulses of energy, delivered rapidly (like a machine gun) and misleadingly added together to give one energy output. It is inferior and much cheaper to produce than an active Q switched laser.
A full medical consultation is essential for diagnosis, confirmation and exclusion of pigment problems associated with malignancy such as melanoma. At our Cambridge Laser Clinic all consultations for pigmented lesions are carried out by a doctor.